


Fig. 1. Male reproductive systemshowing the location of epididymis and vas deferens
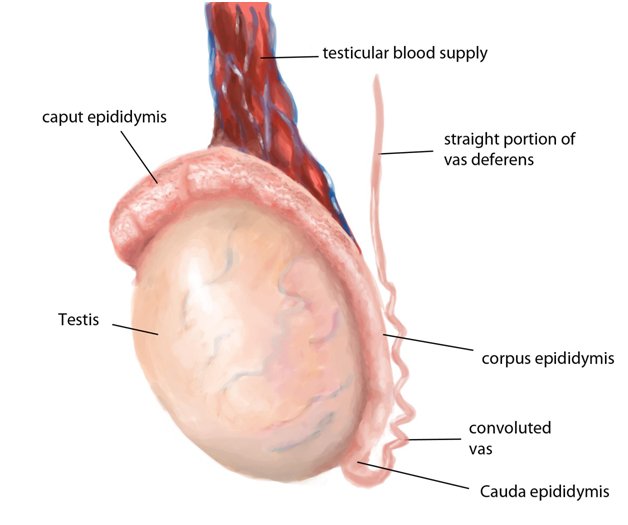
Fig. 2: Different parts of epididymis
Epididymis:
The epididymis is a comma shaped, elongated structure composed of a single, fine tubular structure estimated up to 6 meters (approximately 20 feet) in length. Located on the posterior border of the testis, it is composed of 3 parts, including the head (caput), body (corpora or corpus), and tail (cauda). The epididymal head overhangs the upper pole of the testis, receives the seminal fluid from the ducts of the testis (which pierce the upper portion of the mediastinum), then allows the passage of the sperm into the distal portion of the epididymis. Due to its length, the epididymal duct allows space for storage and maturation of sperm. The maturation of the sperms occurs in the caput region of the epididymis while sperm storage occurs in the cauda region of the epididymis.
Vas deferens:
The vas deferens is a muscular tube roughly 30cm long. It acts as a passage between the epididymis (a coiled tube located at the back of each testicle) and the prostate where semen is ejaculated from during sexual climax. From the prostate the semen is then ejaculated out of the penis via the urethra. Only about 2% of the semen comes from the testicles via the epididymis and vas deferens, but this percentage contains all the sperm necessary for impregnation. Therefore, when the vas deferens is cut (vasectomy), the volume of fluid ejaculated is roughly the same, however, it contains none of the vital sperm.
Causes of vasal obstruction:
Vasectomy: It is the most common cause of vasal obstruction. Vasectomy is a common surgical procedure for permanent contraception in men. It involves cutting and blocking the vas deferens – a tube located in the groin that carries sperm from the testicles to the penis. Vasectomy is a relatively simple procedure. Patients are given general anaesthetic. The urologist then makes two small incisions in the scrotum. Through these openings the two vas deferens are cut and a small piece is removed. The ends of the vas deferens are then tied, stitched or sealed. The scrotum is then stitched up. The whole procedure takes about 15-30 minutes.

- Iatrogenic injury during surgical procedures (eg, herniorrhaphies)
Causes of epididymal obstruction:
- Post-vasectomy associated epididymal obstruction: An epididymal obstruction following vasectomy is the most likely cause of an epididymal obstruction. The buildup of high intraluminal pressures within the epididymis after a vasectomy can result in rupture of the delicate epididymal tubule, resulting in obstruction (eg, epididymal blowout). This phenomenon is more common in men who desire a reversal more than 10 years after their vasectomy and in patients in whom vasovasostomy has previously failed
- Congenital epididymal obstruction:This is usually associated with a cystic fibrosis genetic mutation, and these men may have no other phenotypic manifestations of cystic fibrosis. Some of these patients have a normal vas deferens and dysjunction of the vas deferens with the epididymis
- Inflammatory obstruction of the epididymis: Inflammatory obstruction of the epididymis can result from infections due to some sexually transmitted diseases caused by bacteria like Neisseria gonorrhoeaewhich usually affects only the distal epididymis.
- Traumatic obstruction of epididymis: Trauma to the epididymis is a relatively uncommon cause of an epididymal obstruction but may result from epididymal injury during scrotal surgeries (eg. testis biopsy).
Obstructive azoospermia
Azoospermia is defined as complete absence of sperm from the ejaculate. Although there are many causes of azoospermia, obstruction of the ductal system is responsible for approximately 40% of cases. Obstructive azoospermia may result from epididymal, vasal, or ejaculatory duct pathology.Men with obstructive azoospermia may father children either by 1) surgical correction of the obstruction, which may produce pregnancy by intercourse and obviate the need for assisted reproductive technology; or 2) retrieval of sperm from the male reproductive system for in vitro fertilization/intracytoplasmic sperm injection (IVF/ICSI).
Surgical treatment
Surgical correction may be accomplished by microsurgical reconstruction of the vas and/or epididymis or, in cases of ejaculatory duct obstruction, by transurethral resection of the ejaculatory ducts (TURED). Prior to performing microsurgery in the male, the female partner should be evaluated to determine if female infertility factors are present.
Microsurgical reconstruction of the reproductive tract
Microsurgical reconstruction of the reproductive tract often is successful in patients with obstructive azoospermia. Following vasectomy reversal, for example, return of sperm to the ejaculate occurs in 70-95% of patients, and pregnancies are obtained without the need for assisted reproduction in 30-75% of couples. A very important factor influencing the likelihood of sperm returning to the semen and of pregnancy after vasectomy reversal is the number of years between vasectomy and attempted reconstruction. The length of the obstructive interval and the chance for successful outcome of vasectomy reversal are inversely related. Other factors influencing the success of vasectomy reversal include: the presence or absence of sperm in the intraoperative vas fluid; the gross appearance of the vas fluid; the quality of the sperm in the vas fluid; the length of the vas segment between the epididymis and the vasectomy site; and the presence or absence of a sperm granuloma at the vasectomy site. The likelihood of pregnancy after vasectomy reversal is also heavily influenced by the age of the female partner.
Vasovasostomy (VV) and vasoepididymostomy (VE) are surgical procedures designed to bypass an obstruction in the male genital tract. These procedures are usually performed to restore fertility, although they are occasionally undertaken to relieve pain, such as in postvasectomy pain syndromes.
Vasovasostomies are indicated for an obstruction at the level of the vas deferens, while vasoepididymostomies are used to treat epididymal obstructions. The site of obstruction can often be discerned by examination of the fluid from the vasal end or from the epididymal tubule. The goal of both procedures is to restore genital tract patency and ultimately to allow conception. These procedures are not indicated for nonobstructive causes of azoospermia.
Vasovasostomy involves the anastomosis of segments of the vas deferens above and below an obstruction. The vast majority of vasovasostomies are performed to reverse a prior vasectomy, but the procedure is occasionally indicated for repair of an iatrogenic vasal injury secondary to prior surgery (eg, inguinal herniorrhaphy).
Vasoepididymostomy is a technically more demanding procedure than vasovasostomy. It involves anastomosis (surgical connection) of the vas deferens to the epididymis in order to bypass an epididymal obstruction. This obstruction may be secondary to long-standing vasal obstruction resulting in damage to an epididymal tubule (epididymal blowout) or may result from epididymal infections or trauma

Vasoepididymostomy is performed for congenital, infectious, postvasectomy or idiopathic epididymal obstruction. Following this type of microsurgery, 20-40% of couples achieve pregnancy through intercourse. Accuracy and delicacy of microsurgical technique affect the outcome of reconstructive procedures on the male reproductive system.
Sperm retrieval and cryopreservation may be performed at the time of microsurgical reconstruction in order to avoid a second procedure if the microsurgical reconstruction does not reverse a patient’s azoospermia.
Transurethral resection of the ejaculatory ducts
The possibility of ejaculatory duct obstruction should be considered in the differential diagnosis of obstructive azoospermia.Transurethral resection of the ejaculatory duct results in the appearance of sperm in the ejaculate in about one-half to three-fourths of cases. The pregnancy rate achieved by this surgery is about 25%.
Indications for VV and VE:
- The indications for a vasovasostomy include vasectomy reversal and relief of postvasectomy pain syndrome. The latter indication is uncommon and remains of controversial efficacy. Prior to undertaking a vasovasostomy for vasectomy reversal, the female partner should be evaluated by a gynecologist to exclude concurrent female causes of infertility. Prior to undertaking a vasovasostomy for vasectomy reversal, the female partner should be evaluated by a gynecologist to exclude concurrent female causes of infertility.
- A vasoepididymostomy is performed for the treatment of a genital tract obstruction at the level of the epididymis.
Patients must have active sperm production in the testes to be considered a candidate for a vasoepididymostomy. For this reason, a testis biopsy is usually performed at the time of or prior to planned reconstruction to document active spermatogenesis.